If a vascular stent can penetrate a person's blood vessels, why not just use the stent to suck out the blood clots from the vessels?
Many family members or friends who have had stents put in, mention the question: if you can put a stent in, why don't you draw blood out of the clot?
There are a lot of misconceptions here:

Not all stented vessels have clots.2 Stenting and aspiration are two different techniques.3 Some clots can indeed be aspirated, but only some, and even after aspiration, a stent may be necessary.4 The big data on cardiac thrombotic disease tell us that aspiration is not the best option for the majority of thrombotic disease.
Next, we'll answer each of these misconceptions:
A blood vessel with a stent in it does not necessarily have a blood clot

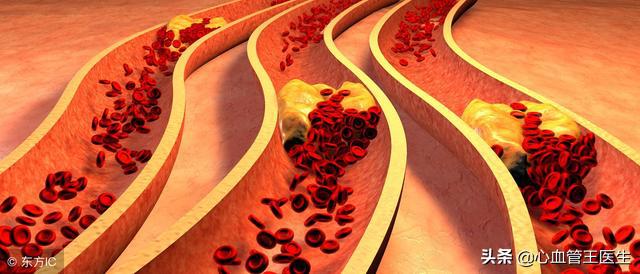
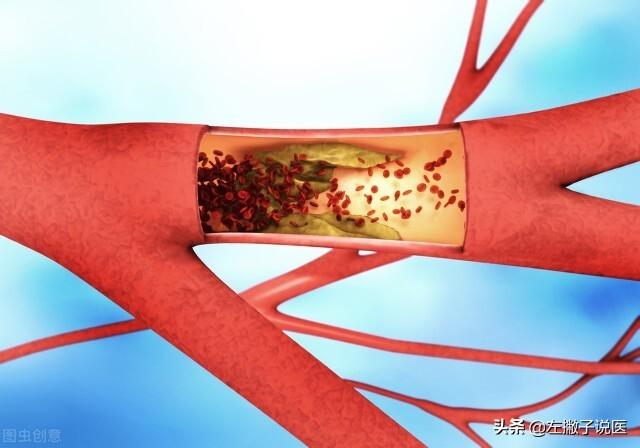
The most common stent is the cardiac stent, of course, now also includes the carotid artery, peripheral vascular stent, renal artery stent and so on and so forth. Let's take cardiac stent as an example, when the stenosis of the heart's blood vessels exceeds 80%, most of the medication at this time is ineffective, not only will recurring angina, for the unstable plaque, because of angina ischemia attack, may also lead to plaque rupture, thrombosis, triggering myocardial infarction, so, at this time, need to be stented to control the onset of angina.
This stenotic lesion requires a stent, but there is no thrombus, and without a thrombus, it is natural to talk about aspiration of the thrombus.
II. Stenting and thrombus aspiration are two techniques
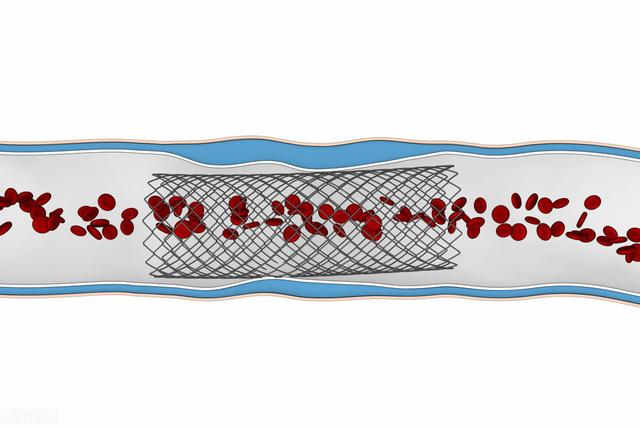
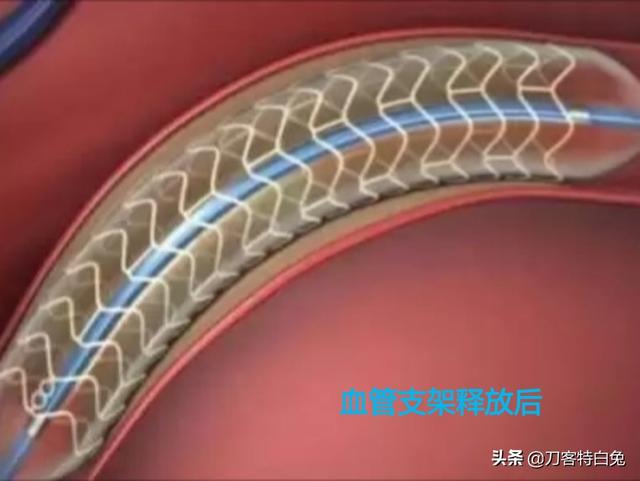
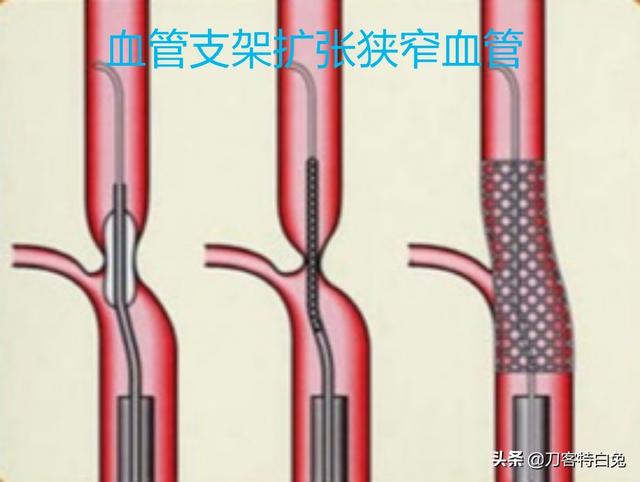
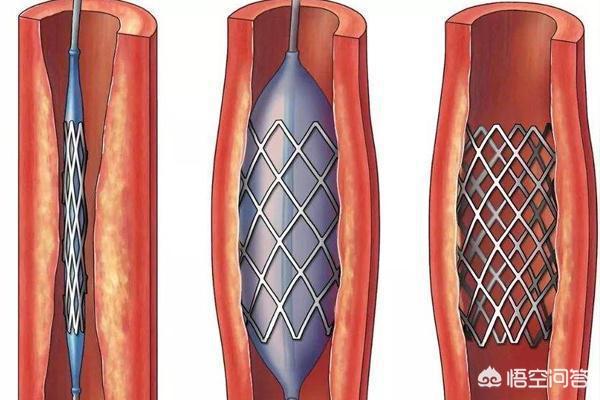
Stenting is simply understood as putting a stent through a catheter into the narrowed part of the blood vessel. At this time, a balloon, as if it were a small balloon, is used to inflate this stent through the inflatable pressure, and the stent will support the narrowed blood vessel, withdraw the balloon, and then the narrowed blood vessel lumen will return to normal, and this is stenting.
Suction of thrombus, again through the catheter, put the catheter opening to the site of the thrombus, at this time, through the negative pressure, that is, suction, then the thrombus will be sucked into the catheter. However, when the thrombus is aspirated, not all of the thrombus can be extracted, the thrombus is a blood clot, the blood clot will not stay in one place, after the catheter touches the thrombus, the thrombus will move, and the big thrombus will turn into a small thrombus, so the aspiration of the thrombus is not as perfect as we all think.
Third, even after suctioning, most of them still have to be stented
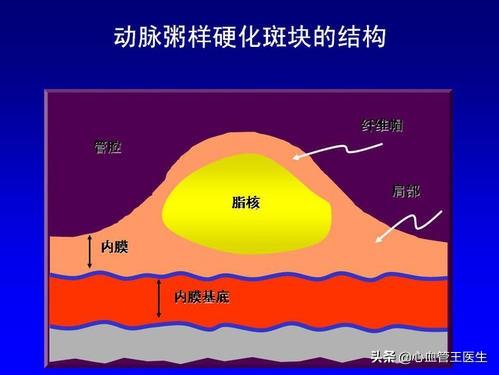
Let's take a step back, even if we could aspirate all the clots and there were no more clots in the vessel, the plaque stenosis would still be there, and the clots are the clots that are formed when the plaque ruptures, that is, the clots that are formed from bleeding in the lining of the vessel. But the plaque stays in the vessel, and even if there is no more thrombus, this fixed stenosis still exists. If it is not stented, then the blood flow will be slow, and not only will you still have angina, but the slow blood flow at the plaque may also lead to thrombosis.
Therefore, for most of the vessels that have undergone aspiration of thrombus, stents may still be needed to support the stenosis so that the official lumen can be restored to normal, angina can be controlled, and prevention of myocardial infarction can be facilitated to a certain extent.
Fourth, the big data tells us that vaping blood clots isn't the best option
Finally, let's look at the big data, the current guidelines for myocardial infarction resuscitation, which come from big data, a lot of case observations that for acute myocardial infarctions, aspiration of the thrombus does not yield better results, that is, aspiration of the thrombus is not as good as not aspirating it, and direct dilatation, stenting, is better for the majority of myocardial infarctions.
Of course in the case of a particularly severe thrombus, it should be pumped, but pumping the thrombus does not mean that a stent is not needed, because although this is a thrombus that caused the myocardial infarction, the fixed stenosis still exists.
In short, medical doctors, scientists, are certainly more bullish than doctors, and doctors follow the guidelines, and in turn aren't those who study medicine more advanced than doctors, more advanced than medical scientists and scientists?
Leave the professional things to the experts, do not worry about it, and do your part is to contribute to the family, society and the country!
Hello! Your question is very thoughtful and a good one. When there is a blood clot blocking a blood vessel, it should be taken out, the clot removed, the blood vessel reopened, and the blood vessel opens up. The reasoning is sound, but there are some questions, and in response to your question, I can give you some answers.
brackets
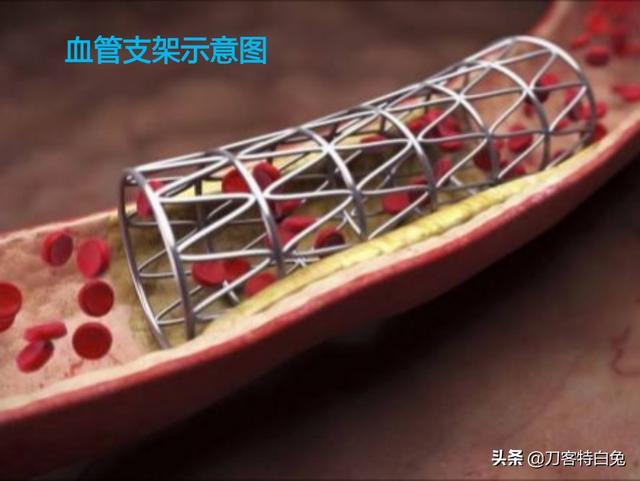
First of all, the function of stents is not to suck up blood clots. The function of vascular stents is in supporting the lumen of the narrowed section of the blood vessel, so that the original narrowed or occluded blood vessel can be reopened and a good blood supply can be restored. It is just like when digging a tunnel, workers need to support the upper and lower ends of the tunnel with sticks and boards in the tunnel. Generally, after the stenosis has been dilated, the blood vessel still cannot be dilated well because of plaque or thrombus, and the blood supply is still poor, then a stent is needed to support the blood vessel wall to achieve the effect of improving the blood supply. Therefore, stents do not have the function of sucking blood clots, stents mainly play a supporting role.
thrombosis
One of the current treatments for intravascular thrombosis, thrombus extraction, is aimed at patients with acute arterial embolism, acute arterial thrombosis, and this group of patients is characterized by - the early stage of thrombosis, that is, the acute stage. It can be treated with thrombus extraction through a Fogarty catheter, which is, you guessed it - sucking out the clot. Or the clot can be removed from the blood vessel by surgical incision. In addition to surgery, there are also medications that can be injected to dissolve the clot away. However, these are only for acute-phase blood clots, and the treatment will be very effective. For chronic thrombus, no matter surgery or drugs, the treatment effect is very poor, it can be said that miss the acute treatment, the thrombus has basically mechanized. To make an analogy, fresh thrombus is like fresh cement, easy to fall off and easy to decompose, and old thrombus is like dried cement, sticking to the wall can't pick off. Therefore, it is almost impossible to surgically remove old, mechanized blood clots from the walls of blood vessels. Surgery can solve many problems, but not all.

Thanks for reading! Please give it a like if you think it's still good, thanks!
Click to follow @杏林锺声 , share a little bit of health knowledge every day to protect your health!
Blood clots can indeed be drawn out! I do not know if you have seen such a news, about a 30-year-old guy, after a dinner party, began to chest pain, stomach pain, vomiting and other symptoms, thought it was too much wine, but tossed the night did not get better, the next morning went to the hospital, the results of the diagnosis of acute infarction, and the left anterior descending branch completely occluded.
The patient was later transferred to the hospital and it was confirmed that the patient's anterior descending branch was blocked by dislodged thrombus and there were also large thrombus formations. Doctors then used a catheter to aspirate the thrombus, and within an hour, six large thrombi were repeatedly extracted, each of which was more than 1cm. People may think, the guy is really lucky, the coronary artery are completely blocked, and still survive, the key is that he just through the thrombus suction cured the disease? The danger of stent surgery was spared.
Is that really true? A blood clot is drawn out, and that's the end of it?

And no!
In fact, the reason that thrombus aspiration is only the first step in an emergency life-saving procedure is because he does have a lot of blood clots in his veins, which would not be treated well if stenting is performed directly. In other words, thrombus aspiration is just the preparation work before the stent surgery. After the guy's thrombus was aspirated, the doctor delivered a drug balloon to his narrowed blood vessels to open them up and restore blood supply to the heart muscle, which completed the treatment. And the drug balloon and stent surgery are actually the same effect. Only the drug balloon's applicability is a bit narrower, maybe the guy is just right for it, which is the best choice considering he is still young.
If a vascular stent can penetrate a person's blood vessels, why not just use the stent to suck out the blood clots from the vessels?
I think we all know a thing or two by the above introduction. Regarding the issue of thrombus aspiration and stenting, both are indeed means of treating acute heart attacks, but they are not substitutes for each other.
Thrombus aspiration cannot be used casually in the clinic; it has specific indications. Existing guidelines recommend that thrombus aspiration should only be used in high-risk acute coronary syndromes with a high thrombus load, that is, in patients with many thrombi at the blocked vessel. As for ordinary patients, it is not recommended. Of course, aspiration of thrombus can be considered in some emergency situations, but it must be done with caution.

Why should thrombus aspiration not be used casually?
- On the one hand, not all patients who need to undergo stenting have thrombus in their coronary arteries, some just have severe stenosis due to atherosclerotic plaque, and thrombus aspiration can only aspirate the thrombus, but for the unstable plaque, it will be dangerous if it is blindly aspirated, and if the plaque is not aspirated, the danger is always there, and there is still a possibility that the vessel will be blocked again. Therefore, even if the standard of load aspiration, after the aspiration of thrombus also need to undergo the necessary stenting surgery.
- On the other hand, thrombus aspiration is also very risky, after all, it is an operation performed inside a blood vessel, it is actually a syringe connected to a catheter and delivered into the blocked blood vessel to forcefully extract the blood clot inside. As you can imagine, pumping from a blood vessel is very dangerous. Moreover, it can only draw out the larger clots, and those smaller clots will be squeezed and may also travel around with the blood flow, causing blockages in other areas. Now there are also studies confirming that thrombus aspiration has no therapeutic advantage. So neither is recommended for clinical use.
In fact, thrombus aspiration is more commonly used in clinical practice for the treatment of cerebral infarcts and is clinically referred to as thrombectomy. However, the surgery needs to undergo a rigorous safety assessment before it can be performed, after all, the risks of the surgery are also high. Even so, thrombectomy is not the first choice for the treatment of cerebral infarction, and intravenous thrombolysis is generally preferred for patients within the time window.
In conclusion, thrombus aspiration does exist, but it is not a substitute for stenting, and it is by no means available to anyone, and it all needs to be decided by a doctor in a comprehensive evaluation as to who can have it done. As a patient, just follow your doctor's instructions!
I am Pharmacist Wang, insisting on spreading the knowledge of cardiovascular and cerebrovascular diseases with simple and easy-to-understand words, and dedicating my own small efforts for a healthy China. If you think my answer is helpful to you, please leave a like it! In addition, if you still have related questions, welcome to leave a message, we discuss together!
In some neurologic acute cerebrovascular diseases, revascularization can be achieved by removing the thrombus, but these cases are acute and severe. For cardiovascular and cerebrovascular accidents with less acute onset, it is elective endovascular stenting. After all, thrombectomy is technically more demanding, more risky than stenting, and more expensive, and is not suitable for all cases.
Greetings! Your question is very thoughtful and the idea is right. There is a blood clot blocking the blood vessel, remove the clot and the blood vessel opens up.This has been done clinically.
The Solitaire FR stent is the specialized thrombolytic stent approved for use in patients undergoing arterial thrombolysis.The procedure for removing the thrombus is relatively simple, starting with a microcatheter and microguidewire through the thrombus. The FR stent is then used to follow the microcatheter through the thrombus. The stent is semi-released, and then the microcatheter and stent are clutched and dragged into the introducer catheter. Drag them out together and you're done.
Anticoagulation is not routinely used after thrombectomy, except in special cases, such as cardiac cerebral embolism, arterial entrapment, and in more unusual cases such as severe endothelial damage after thrombectomy, residual stenosis, secondary thrombosis, etc. Anticoagulation can be done with either low molecular heparin or normal heparin.
Residual stenosis after thrombus removal is common; some patients may not have a thrombus and simply have a vessel occlusion on top of a severe stenosis; in these patients, the removal of a thrombus may not retrieve anything but reveal severe stenosis and hypoperfusion in the responsible vessel, and balloon dilatation or stenting is feasible at this point.
After stenting, stent release, or balloon dilatation, may be considered if the artery is found to be severely stenotic or if the endothelial damage is felt to be severe and may be secondary to the formation of another thrombus.
I'm @KnifeTheWhiteRabbit and I write medical science articles in my spare time, hopefully I can help you. Thank you for your attention and support!
Advances in technology have contributed to making clot clearing a reality. The technology is now available, presumably because stents are too profitable and have been suppressed.
Such a question should be raised because the patient has a misunderstanding of the two treatment techniques of stenting and thrombus aspiration. In fact, stenting and thrombus aspiration are two different treatment techniques. In some patients with blood stenting, there is not necessarily the presence of thrombus, so the two should not be confused. Below, I will talk to you about this issue.
First, let's talk about putting up the brackets
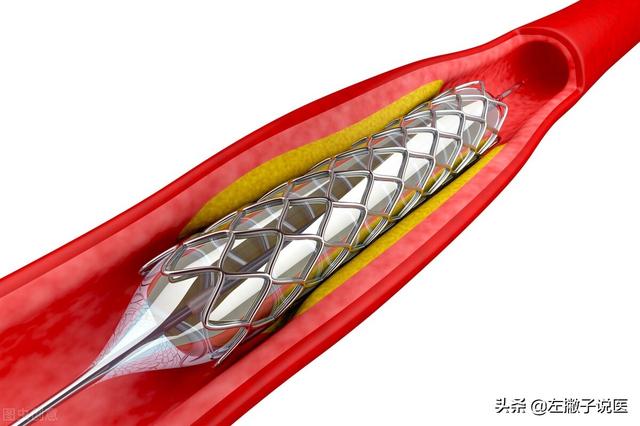
The purpose of placing a stent is to reopen a narrowed or occluded blood vessel by placing the stent into the lumen of the narrowed section of the blood vessel to open it up, thus opening up the originally narrowed or occluded blood vessel, and then the blood flow will return to normal, thus preventing hypoxia and ischemia problems from occurring.
For example, some patients with acute myocardial infarction, moderate to severe angina or unstable angina can be treated with stenting at this time when long-term medication is not ideal. This can save the patient's life in time, but also effectively reduces the attack of angina pectoris, and also reduces the risk of serious or fatal heart disease, so that the patient's quality of life is well improved.
And most of the narrowing or occlusion of this vessel occurs due to the occurrence of atherosclerotic plaque, which can be stabilized with the lumen of the vessel, and normally cannot be suctioned out. So it can only be propped up with a stent so that the channel can be opened.
In addition, in most cases, the narrowing or occlusion of a blood vessel does not necessarily mean that there is a thrombosis problem, only some unstable plaque dislodged and blocked at the narrowed blood vessel, so that blood clots are prone to form.
Therefore, for the occurrence of atherosclerotic plaques caused by the narrowing of blood vessels as well as blockage, there is no thrombus problem at all, and there is no need to talk about aspiration of blood clots. Moreover, stenting is stenting and thrombus aspiration is thrombus aspiration, and the two cannot be performed at the same time.
Next, let's talk about blood clots
A thrombus is a solid mass of blood that has coagulated in a blood vessel or has formed from the clumping of some of the blood's constituents. The thrombus can be divided into white blood clots and red blood clots, white blood clots are platelet thrombosis, containing more platelets, mostly in the arterial blood vessels, can be tightly combined with the blood vessel wall; and red blood clots contain more red blood cells, mostly in the venous blood vessels, the thrombus is relatively soft, easy to dislodge, and can be moved with the flow of blood to other parts of the body in the narrowing of blood vessels are prone to cause embolism.
Therefore, when a thrombus occurs, when the condition is critical, such as patients with acute arterial embolism and acute arterial thrombosis, it is necessary to aspirate the thrombus in time in order to effectively alleviate the patient's symptoms and prevent the patient from having a life-threatening situation in a short period of time. If the formation of multiple thrombus is not timely suction thrombus out, cardiac thrombosis can cause myocardial infarction, cerebral thrombosis will cause aphasia hemiparesis, and even life-threatening in serious cases.
Suction of thrombus is not as easy as we think, and it is even more difficult than stenting. For some venous thrombus, because the blood flow is relatively slow can easily suck out the thrombus, but for some arterial thrombus, because the blood flow is relatively fast, and these clots will not honestly stay in one place, when suctioning the thrombus, these clots will move, and the big clots will become small clots flowing along with the blood to other places. Therefore, it is not possible to aspirate all the blood clots inside the blood vessels, and it can also cause new blockages.
Also, there are some clots that over a period of time become mechanized, that is, they become attached to the walls of the blood vessels, in which case they cannot be suctioned out because they have already adhered to the walls of the blood vessels.
Therefore, this treatment of sucking out blood clots is usually for the acute stage of blood clots, and the effect is also better. But for those who have been connected with the blood vessel wall of the old mechanized thrombus, not only can not be sucked out, even also surgery can not be removed, this time also only through the release of stents can make the blocked blood vessels to restore the smooth flow.
Overall, what we need to know is that stenting and aspiration of blood clots are two different treatment techniques. Not all blood clots can be successfully aspirated, and sometimes even if the blood clots can be aspirated, a stent still needs to be put in place in order to keep the blood vessels open.
Author's note: I am very happy to popularize health-related knowledge for everyone, I am left-handed to say medical, every day in simple language for you to popularize professional medical knowledge, the code word is not easy, if you like my article, please help me point a praise! If you have any questions, you can leave a message in the comments section, welcome to pay attention and forward, thank you for your support!
You mean the wire tubing that passes the stent sucks out the clot, right?
The lineal tube is only one-tenth the size of a blood vessel, and how can a thrombus be inhaled into a narrower lineal tube when the blood vessel is even blocked. Unless it releases a lysate that can be inhaled through the lineal tube, then it's more likely to flow through the blood vessel
There is never a shortage of smart people in the world, and this idea is not unique to you; it has long been used in clinical care, but never in your imagination: removing blood clots through stents.
Stenting is stenting and bolus removal is bolus removal; they are individuals with different concepts and different applications and should not be crossed or abused with each other.
Coronary stenting!
Stenting is a minimally invasive procedure in cardiology that distinguishes itself from conventional cognition and does not require opening of the patient's chest, much less general anesthesia, but only local anesthesia.
The doctor will often make a puncture in the patient's radial or femoral artery and put in a sheath, which is the key to all subsequent operations. In the temporary channel created by this sheath, we put in a guidewire and a catheter (the guidewire is responsible for guiding it) and slowly deliver it to the coronary blood vessel near its opening, and then remove the guidewire to inject a contrast medium (coronary angiography) to determine the degree of coronary stenosis, and then proceed with subsequent The procedure is then performed as needed.
For example, through this catheter, the balloon is placed into the stenosis, and then the balloon is propped up with a pressure pump, which will artificially open the narrowed coronary vessel, and at that point the purpose of dilating the vessel has actually been achieved, but this dilation is only temporary, and understanding that, stenting is much simpler.
A stent is a stent placed outside of the balloon. When the balloon is propped up, the stent will naturally fit on the vessel wall as well, at which point the balloon is withdrawn back out of the vessel and the stent implantation procedure is completed.

Remove the bolus for treatment!
Thrombolysis may seem wonderful, but in reality it has many limitations in clinical application.
The effect of thrombus removal is not as strong as one might think; it is often mentioned only when the thrombus load is more severe, and when it is applied in time, it does not remove the thrombus completely, but only some of the larger clots; the rest of the clots are dislodged and travel with the blood flow, blocking other blood vessels.
And it is not always the case that patients who need stents have blood clots. In addition to the conventional sense of plaque thrombus blockage of blood vessels, there are some patients who do not have the presence of plaque thrombus, there is still a serious stenosis blockage, they may be due to abnormal nerve discharges leading to spasm contraction, for this situation is more serious patients, there is no embolism can be desirable, naturally, you can not blindly apply.
This is by no means an isolated case, there are many clinical variables, it's not a case of not doing it but not being able to do it, there is no treatment measure that applies to everything, only what is reasonable to apply, trust your doctor.

I hope my answer will help you!
If there's anything you don't understand, comment and private message me!
Think of it as unclogging a drain. Blood clots are the symptom, the cause of formation is the cause . ...... I can't make it up.
This question and answer are from the site users, does not represent the position of the site, such as infringement, please contact the administrator to delete.